A team of nurses and physicians from OHSU in Portland, OR, our mission is two weeks of treating local women with uterine prolapse, a debilitating pelvic anomaly resulting from weakened pelvic muscles causing the uterus to slip down, or even out of, the birth canal. Eight hours in a van, dodging potholes in a hard-packed dirt road, motoring westward from the capital city, Addis Ababa while our potential patients are walking for hours then riding a bus even longer to get to Gimbie. Word spreads fast. Nearing Gimbie the terrain changes as we climb in altitude.Out the window of the van: perhaps he is nine years old, maybe less, but he is his family’s livestock manager. Daily, the livestock must graze, often far from home.
Gimbie Adventist Hospital is located in Gimbie Town, approximately 450 km west of Addis Ababa, Ethiopia. Gimbie itself is located at an altitude of approximately 2000 meters. Down a shady, lightly-traveled path off Gimbie’s main street, itself a dirt road, the team from Portland OR caught a first glimpse of the hospital.
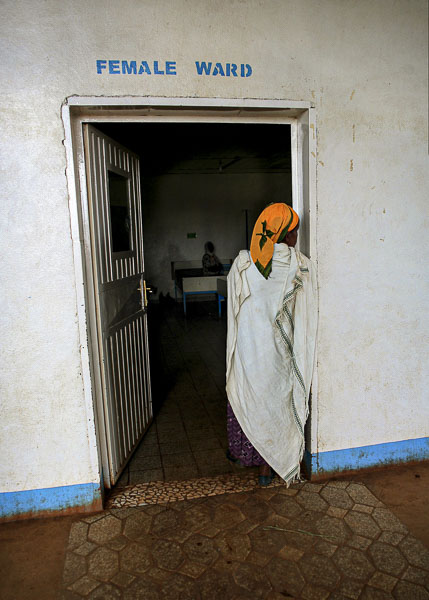
Through the hospital’s maze of halls, we exited at the rear where we could see our main quarters, The Surgeons’ House, down the steep hill. Home away from home for two weeks, where some would sleep, all would eat and gather for team meetings.Within forty-eight hours, our first patients were gathering in the Clinic for evaluation. Word of our plans for surgery was disseminated via radio, accessible to a large number of people in the area, a vast area.Elegant and poised, this young woman has delivered 5 children, working throughout her pregnancy and almost immediately following childbirths. Her uterine prolapse is pronounced and limiting her daily life.Older, confident, very tall, and strong, this woman was happy to pose for me, and pose she did! She has lived with a prolapsed uterus for years, working in her home and fields .Her heart is breaking. A prolonged labor of five days duration has left her with a pelvic injury, a fistula. This hole connects her bladder and her vagina leaving her unable to control the flow of her urine. The ongoing incontinence leaves her skin excoriated down her legs, all the way to her feet, her body and living area smelling of stale urine. Fistula patients are most often rejected by their husbands, families and village, leaving them to a life of rejection and isolation. She is our only Fistula patient in this Mission, planned for treating uterine prolapse.African women rarely speak English, for a variety of cultural reasons, and therefore depend upon the men in their families, among whom English-speakers are more common. Gentlemen like these serve as interpreters for their loved ones and eagerly help others in the ward who need help.The Female Ward. All our patients are admitted the night before surgery, given access to a bath and a bed for an overnight rest following the long trek to Gimbie. Travel-weary family members sleep in the same bed, exhausted. In the next bed? The same story. There are twelve beds in each of two women’s wards.We explore the operating suite to get familiar. This substandard , but functional , facility is the only hospital for miles.There are no laundry facilities in the hospital, therefore there are no sheets, rather plastic covers that are cleaned between patients with disinfectant.Dr. Larson, an anesthesiologist, working under a number of serious challenges. One? Using the anesthetic vaporizer for a specific drug to vaporize a different drug, a serious dosing challenge.Our local colleagues: full time staff of the Operating Rooms: Housekeepers, Orderlies, Nurses and the only Nurse Anesthetist covering this Clinic’s surgical needs.In this Faith-based hospital, pastoral care is offered daily for patients and their families by American missionaries.Born dramatically premature, this baby girl was abandoned. Her mother left the hospital as soon as she could walk saying she had other children who demanded her care. She told the nurses she could not care for a baby with such needs. And then she was gone. The infant has a gastric tube for feedings but was not thriving by the time we finished our work here.Exploring the grounds, I met these two women, both locals, who volunteer at the hospital.And near the Surgeons’ House, another local woman roasts coffee in a dedicated space, an exacting and time-consuming art. We took advantage of her talent for coffee during our stay as well as to pack for our return to the US.Breakfast! Homemade bread crafted expertly by our cook , more than making the rustic quarters feel more like home.Our first morning, thick oatmeal, hot coffee. Napkins improvised.Time to get started. The first day’s team meeting over breakfast, with a view from the balcony of the “Surgeons’ House”.The view.Our post operative ward and an impromptu staff conference.This young boy was struck by lighting, suffering extensive exit wounds. His mother had to return to her other children and left him at the hospital where he undergoes frequent debridements and bandage changes under sedation in the operating room. His prognosis is good. We all hope she returns for him.Nursing students from a local school spent time with our nursing staff, absorbing every possible clinical experience. Working at OHSU, our RNs were adept at teaching trainees.The newest Ethiopian takes her first breaths having been delivered by an urgent Caesarian Section, the most commonly performed surgical procedure in this and most rural Ethiopian Hospitals.Under General Anesthesia in the main operating room, women hoping for more children are treated for uterine prolapse with preservation of their reproductive options.Under general anesthetic she wears her house keys around her neck along with a religious charm.In the second operating room ( never used due to lack of staff and lack of basic equipment) we set up for spinal anesthetics using monitoring devices brought from the US, purchased at Walgreens: basic and functional.Intra Op. Her spinal anesthetic is working; she is comfortable and sedated only minimally. At last she is relaxed, believing for the first time maybe, that her decision to walk to Gimbie would not cost her her life. The majority of women tell us that they are here because Uterine Prolapse had taken its toll, that life was no longer worth living with this disability, this affliction. They were willing to risk death during surgery in hopes they could be could be made whole.Intra-operatively. Calm, under a spinal anesthetic.
Years of carrying wood for miles beginning at a young age has changed the contour of her spine. While subtle to a casual observer, the curve is dramatic to the person hoping to place a spinal anesthetic.Bending under the weight of the wood, they are often cut by the sharp edges of the dry branches.All in a Day’s work for Ethiopian women and girls.Teaching is a major piece of this Mission directed to surgical residents from both Portland, Oregon, and the region around Gimbie. Here Dr. Osmundsen is treating uterine prolapse in an elderly woman with a vaginal hysterectomy under a spinal anesthetic.The Gimbie Adventist Hospital has no nurses to work in a Recovery Room; we staffed ours with top notch professionals from OHSU, the standard of care for surgical patients in the US.Our team’s post operative Ward is the re-purposed Auditorium, spacious but on the top floor. Team effort is key.Three generations of Ethiopians.An attentive brother joined his sister, walking to Gimbie with her, then sitting nearby as she recuperated for two days.Joy. The look on her face when she regained consciousness told us: She was dry. She knew before we did, but we knew when we saw her face. In closing the fistula, the hole communicating between her bladder and her vagina, there was no more leak. She felt the dryness. She was no longer incontinent. What this meant to her was immeasurable.Nestled under the coverlet her son brought with them along the journey to Gimbie. He sat at her bedside for two days.Exhausted, left with no facilities for family members, a man, a brother, sleeps when he can on this sofa missing its cushion.Early morning rounds on all patients whose surgery had been completed in the previous days. Unlike in the US, curious onlookers often observed, over our shoulders.Husband and wife, two days post-op. Relieved, joyful.On the third post op day, most patients were ready to start the journey homeward, accompanied by loved ones and wearing a new pair of shoes donated by Keen Shoes of Portland. This woman wears the tattoos along her jawline given her at puberty , a rite of passage into womanhood and a tribal tradition. Her son is ready to walk her home.She took a risk walking to Gimbie to put herself into the hands of strangers from America . Today? She is whole.